

 Alkaline Phosphatase
Clinical Biochemistry in Primary Care
Creatinine Kinase
Hyperkalaemia
Hyperlipidaemia
Hypomagnesaemia
Lipid A&G Service
Breast A&G Service
Axillary masses
Breast Implants (non-cancer)
Breast Pain
Breast Surgery
Breastfeeding
Family History of Breast Cancer
Male Breast Symptoms
Mastitis and Breast Abscess
Nipple conditions
Bowel Cancer Screening
Breast Cancer Screening
Cervical Cancer Screening
Pancreatic Cancer Surveillance Programme
Lung Cancer Screening (LCS)
Cancer Support A&G Service
Cancer and Severe Mental Illness (SMI)
LD & Cancer
Living with and beyond cancer (LWBC)
Nutrition in cancer
Physio for NBT Cancer patients
Post cancer - Digital Remote Monitoring and Personalised Stratified Follow Up
Exercise programmes for people affected by cancer
Toxicity Risk Assessment Tool
Cardiology A&G Services
Angina
Arrhythmia
Atrial Fibrillation and Flutter
Cardiac Rehabilitation
Cardiac Rhythm Analysis
Coronary Artery Calcification
ECG - Open Access
ECHO - requesting
Heart Failure
Hypertension
Infective Endocarditis
Inherited Cardiac Conditions
NT Pro BNP Testing
Pacemakers
Postural Orthostatic Tachycardia Syndrome (PoTS)
Pulmonary Hypertension
Rapid Access Chest Pain Clinics
Syncope and TLOC (non-traumatic)
Thoracic Aorta Disease
Care of the Elderly A&G Service
Assistive Technology Service
Falls & Balance
Fracture Liaison Service
Frailty
Hearing Services
Live Longer Better
Movement Disorders
NHS@home - Frailty pathway
Rapid Assessment Clinic For Older People
Referral pathways for older people
Acute Assessment
COVID Medicine Delivery Unit (CMDU)
COVID Oximetry @ Home Virtual Ward
COVID Testing
Long COVID
TeamNet and Latest updates
Dementia - Assessment & referral
Dementia Prescribing
Mental Capacity & Best Interest Decisions
Mild Cognitive Impairment (MCI)
Acne vulgaris
Actinic Keratoses
Dermatology A&G Services
Alopecia
Basal Cell Carcinoma
Benign Skin Lesions
Bowen's Disease
Community Dermatology Service
Cosmetic skin treatments
Eczema
Hidradenitis Suppurativa
Hyperhidrosis
Leg Ulcer
Mole Mapping/Surveillance
Pityriasis Rosea
Pityriasis Versicolor
Polymorphic Light Eruption
Pruritis
Psoriasis
Rosacea
Scabies
Seborrhoeic Dermatitis
Skin Camouflage
Tinea
Tissue Viability/Wound Care Service
Appearance-Related Concerns
Urticaria
Vulval Skin Care
Warts and Verrucas
Community Diabetes Specialist Service
Diabetes & Nutrition
Diabetes A&G Services
Diabetes Foot Care
Diabetes Mellitus - Guidelines
Diabetes self-management
Diabetes Structured Education
Diabetic Eye Screening
Monogenic Diabetes
Neuropathic Pain (Diabetic)
Non-diabetic Hyperglycaemia and the National Diabetes Prevention Program
Pregnancy and diabetes
Rapid Access Diabetes Clinic
Type 2 diabetes management
Type 2 Path to Remission Programme
Dietetics & Nutrition A&G Service
Local Services
Malnutrition & Oral Nutritional Supplements
Vitamin D Deficiency
Weight management
Alcohol Misuse
Opiate Dependence
Non-opiate drug dependence
North Somerset Drug & Alcohol Service
South Gloucestershire Drug & Alcohol Service
Bristol Drug and Alcohol Service
Bristol Primary Care Liaison (formerly Shared Care)
Bereavement support
Death Certification and Medical Examiner
End of Life Care
End of life care - community support
ReSPECT Plus
SR1 Form (formerly DS1500)
St Peters Hospice
Weston Hospice
Adrenal incidentaloma
Adrenal insufficiency
Endocrinology A&G Service
Endocrinology Services - UHBW and NBT
Gynaecomastia
Hirsutism
Hyperprolactinaemia
Hyperthyroidism
Hyponatraemia
Hypothyroidism
Male hypogonadism
Managing glucocorticoid withdrawal
Polyuria
Primary hyperparathyroidism (PHPTH)
Secondary hypertension
Sub Clinical hyperthyroidism
Sub Clinical hypothyroidism
Thyroid Disease and pregnancy
Thyroid eye disease
ENT A&G Service
Anosmia
Audiology (adult)
Dizziness and Vertigo
Ear wax and microsuction
ENT HOT Clinic
Epistaxis
Hearing Problems
Middle ear problems
Moulded Ear Plugs
Nasal Treatment
Neck Lumps (including Goitre)
Otitis Externa
Rhinosinusitis & Nasal Polyps
Snoring
Speech & Language
Tinnitus
Tonsils
Uvula
Advice and Guidance - Gastroenterology and Colorectal Surgery
Anaemia (Iron Deficiency)
Anal FIssure
Barrett's oesophagus
Coeliac Disease
Colon Polyps
Community Gastroenterology Clinic - InHealth
Constipation in Adults
Diverticular Disease
Dyspepsia and Reflux
Endoscopy
Eosinophilic Oesophagitis
Faecal Calprotectin
FIT (Faecal Immunochemical Test)
Gallstones (and polyps)
Haemorrhoids and anal lesions
Hiccups
Inflammatory Bowel Disease (Confirmed)
Inflammatory Bowel Disease (suspected)
Irritable Bowel Syndrome
Microscopic Colitis
Pancreatitis (Acute)
Pancreatitis (Chronic) and PEI
Rectal Bleeding
Stoma care
Upper GI Bleed
Urgent Gastroenterology Services
Alpha 1 Antitrypsin Deficiency (AATD)
Family History of Colorectal Cancer
Genetic Haemochromatosis
Genetics - general
Lynch Syndrome
Monogenic Diabetes
Family History of Breast/Ovarian Cancer
Abnormal Vaginal Bleeding
Gynaecology A&G Service
Cervical Conditions
Dyspareunia
Early Pregnancy Assessment Clinic
Emergency Gynaecology
Endometriosis
Female Cosmetic Surgery
Female Genital Mutilation
Female Genitalia Surgery
Female Urinary Incontinence
Fibroids
Hyperemesis Gravidarum
Menopause
Menstrual Disorders
Mesh Complications
Open Access Gynae Imaging
Ovarian Conditions
PCOS
Pelvic Inflammatory Disease
Pelvic Organ Prolapse
Persistent Pelvic Pain (women)
Premature Ovarian Insufficiency
Recurrent Miscarriage
Termination of Pregnancy
Vulval Skin Conditions
Haematology A&G Service
Anaemia
Blood Transfusions & Iron infusions
Genetic Haemochromatosis
Guidelines for Primary Care
Leucocytosis (including neutrophilia and lymphocytosis)
Lymphadenopathy (adults)
Macrocytosis
Polycythaemia
Sickle Cell & Thalassaemia
Vitamin B12
Warfarin monitoring
Hepatology A&G Service
Genetic Haemochromatosis
Liver disease
Urgent Hepatology Service
Viral Hepatitis
Advice & Referrals - Infectious Diseases and Microbiology
Antimicrobial Guidelines (Primary Care)
Clostridioides difficile in the community
COVID -19 (Coronavirus)
Group A Strep
Helicobactor Pylori
Immunisation Schedules
Infection Sciences Test Sample Quick Guide
Influenza
Lyme Disease
Malaria
Measles
Mpox
Mumps
Public Health and Notifiable Diseases
Syphilis
Tuberculosis
Varicella
Vector Borne Diseases
Viral Haemorrhagic Fever (incl Ebola)
Whooping Cough
Middle Eastern Respiratory Virus - MERS-CoV
Biochemistry Advice
Chronic Disease Monitoring
Community Diagnostic Centres
Community phlebotomy
Inflammatory Marker Testing
Medical Calculators
Transport and storage of samples
Pathology Services
Adult Learning Disability Health Service
Constipation and Learning Disability
Dyslexia
Dyspraxia / DCD in adults
LD & Autism Hospital Liaison
LD & Cancer Screening
LeDeR - learning disability mortality reviews
Mental Capacity & Best Interest Decisions
Resources for Learning Disability Annual Health Checks and Health Action Plans
Stop over medication (STOMP)
Max Fax and Dental A&G Service
Cleft Lip and/or Palate (adult)
Dental Care
Reconstructive Prosthetics Services
Salivary Gland Problems
Temporomandibular Joint Disorders
Trigeminal Neuralgia
Alternatives and Adjuncts to HRT
Cardiovascular conditions and HRT
Contraception and Menopause
Diagnosing menopause
Early menopause - under 45
Genitourinary symptoms
Gynaecology conditions and HRT
Hormone Replacement Therapy (HRT)
HRT and breast conditions
HRT and Migraines
HRT in over 60s
Hormone sensitive cancers
Post-menopausal bleeding - not on HRT
Premature Ovarian Insufficiency (Menopause <40y)
Referral - Menopause
Side effects and risks of HRT
Testosterone for low libido
Unscheduled bleeding on HRT
VTE and HRT
Resources for patients
24/7 Mental Health Support
ADHD (adult)
Autism-Spectrum
Depression (adults)
Eating Disorders
Gambling Addiction
HOPE programme
ICU Follow-up NBT
Insomnia
MINT (Mental health and wellbeing Integrated Network Team)
Mental Health - Social Prescribing
Mental Health Support - Which Service
Neuropsychiatry
Perinatal Mental Health
Primary Care Liaison Service - AWP
Psychosis: Schizophrenia
Safe Haven Mental Health Support
Sanctuary (Bristol) Mental Health Support
Second Step Wellbeing Services
Self Harm
Self-help Leaflets for Mental Health
Sexual Assault / Abuse Support
SMI (Severe Mental Illness) Physical Health Improvement
Suicidal Thoughts
Talking Therapies (IAPT)
Coping With Appearance Concerns
Veterans Mental Health
Right to Choose (ADHD/ASD Patient Choice)
Nephrology A&G Service
Acute Kidney Injury
Chronic Kidney Disease
Renal referrals (including urgent referrals)
Neurology/HOT Clinic A&G Service
Neurovascular/Stroke A&G Service
Bell's Palsy
Cognitive Disorders
Concussion / mild traumatic brain injury
First Seizure Clinic
Head Injury Therapy Unit
Headache (adults)
Huntington's Disease
Multiple Sclerosis
Neuromuscular
Neurophysiology
Neuropsychiatry
Parkinson's Disease
Peripheral Neuropathy- Under Review
Restless Leg Syndrome
Spasticity service
Specialist Community Neurology
Stroke
Transient Ischaemic Attack
Tremor
Trigeminal Neuralgia
Neurosurgical Referrals - General
Arachnoid cysts
Brain Conditions
Cauda Equina Syndrome
Epilepsy surgery and DBS
Normal Pressure Hydrocephalus
Peripheral Nerve Conditions
Spinal Conditions
Subdural Haematoma
Trigeminal Neuralgia
Obstetrics A&G Service
Cholestasis of Pregnancy
Diabetes in Pregnancy
Early Pregnancy Assessment Clinic
Family Nurse Partnership
Folic acid and Vitamin B12 in pregnancy
Group B Strep in Pregnancy
Hyperemesis Gravidarum
Hypertension in pregnancy
Maternity Services
Perinatal Mental Health
Post Natal Care
Termination of pregnancy
Thyroid Disease and Pregnancy
Vaccination in Pregnancy
Acute Angle Closure Glaucoma
Ophthalmology A&G Service
Allergic Eye Disease
Anterior Uveitis / Iritis
Blepharitis
Cataract
Chalazion & Styes
Chemical injury
Conjunctivitis
Contact Lens Related Keratitis (Corneal Ulcer)
Corneal Abrasion
Corneal Foreign Body
Dry Eye
Endophthalmitis
Episcleritis
Eyelid conditions
Floaters & Flashes
Giant Cell Arteritis
Glaucoma
Hyphaema
Low Vision
Neuro-ophthalmology
Open Eye Injury
Ophthalmic Shingles
Orbital Trauma / Suspected Orbital Fracture
Pingueculum & Pterygium
Pre-septal and Post-septal Cellulitis
Referral Guidance & Tips
Subconjunctival Haemorrhage
Urgent Ophthalmology Referrals
Acute knee & shoulder clinics
Orthopaedics A&G Service
Back pain/ Spinal pathway
Carpal Tunnel Syndrome
Dupuytren's Contracture
Foot and Ankle Problems
Fracture Clinics
Funding Policies for Orthopaedics
Ganglion
getUBetter app
Hand problems
Hip Pain
Knee Pain
Meralgia Paraesthetica
MSK Foot & Ankle service
Musculoskeletal (MSK) self-help
Musculoskeletal Interface (MSKI) Service
Periprosthetic hip infection
Shoulder Problems
Sports Injuries
Steroid injections
Trigger Finger
Acupuncture
Pain Management A&G Service
Back Pack
Fibromyalgia
ME/Chronic Fatigue Syndrome
Persistent (Chronic) pain
Spinal Cord Stimulation Service
Physiotherapy A&G Service
Divarication of Recti
MSK Physio services
Neurophysiotherapy
Pelvic Health Physio
Respiratory Physio
Self-management Hip & Knee pain
Alternative Medicine
Antibiotics
Cannabis prescribing
Community Pharmacy
Hosiery
Medication to avoid in dementia patients
Medicines for Self Care
Medicines Quality and Safety
NHS@Home - IV antimicrobials (OPAT)
Opioid Conversion
Prescribing in pregnancy and breastfeeding
Psychotropic Medication Monitoring
Toxbase
Vitamin D
Advice & Queries
Direct Access Radiology (adults)
ICE System for Radiology (& Pathology) Referrers
Image Guided Steroid Injections
MRI considerations
Radiology Guidelines for Primary Care
Spinal Imaging in Primary Care
Ultrasound guidance
Respiratory A&G Service
Air pollution and health
Asthma (adults)
Breathing Pattern Disorders
Bronchiectasis
Chronic Breathlessness Support
Chronic cough
Chronic Obstructive Pulmonary Disease
Community Respiratory Service
Fit to Fly Assessments
Home oxygen ordering
HOT Clinics (Respiratory)
Interstitial Lung Disease
Long-term Ventilation (LTV) Service
myCOPD App
NHS@home - Respiratory pathway
Obstructive Sleep Apnoea
Pleural Services
Pulmonary Rehabilitation
Respiratory Triage Services (RAS)
Smoking Cessation
Spirometry and Lung Function Tests
Tuberculosis
Lung Cancer Screening (LCS)
Rheumatology A&G Service
Axial Spondyloarthritis (including ank spond)
Early Inflammatory Arthritis
Fibromyalgia
Giant Cell Arteritis
Gout (Crystal Arthropathy)
Hypermobility and EDS
Osteoporosis
Osteoporotic Vertebral Fracture
Polymyalgia Rheumatica (PMR)
Psoriatic Arthritis (PsA)
Raynaud's Phenomenon
Sjorgren's Sydrome
Systemic Lupus Erythematous
Young Adult Rheumatology Service
Adult Safeguarding
BNSSG Safeguarding Team & Training
Domestic Violence and Abuse
Sexual assault/ abuse support
PREVENT
Better Health North Somerset
Exercise on referral
HOPE programme
Live Longer Better
Musculoskeletal (MSK) self-help
South Gloucestershire
Self Care
Smoking Cessation
Sexual Health A&G Service
Chronic Pelvic Pain Syndrome (men)
Contraception
Emergency Contraception
Gonorrhoea
HIV
LARC
LARC Complex referrals
Loss of Libido
Mpox
Pelvic Inflammatory Disease
Post Birth Contraception
Psychosexual Service
Sexual assault/ abuse support
Sexual Health Guidelines and Referral
Syphilis
Circadian Rhythm Disorder
Insomnia
Obstructive Sleep Apnoea (OSA)
Parasomnias
Primary Hypersomnias
Restless Leg Syndrome
Advice & Guidance Service
Cosmetic Treatment (including scar revision)
Foreign Body Removal (soft tissue)
Hernias (adults)
Burns (adult)
Pre-operative assessment
Reconstructive Prosthetics Services
Surgical Emergency Care
Admission protocols
Dementia Wrap Around Care - North Somerset
Frailty - ACE
Frailty - Urgent Care
HOT Clinics & Rapid Access
Live UEC Dashboard
Medical Assessment/Admission and Weekday IUC Professional Line
NHS@home
Septicaemia (adults)
Sirona Professional Lines
Surgical Emergency Care
Transport to Hospital
Urgent Care, MIU & WIC
Urgent Community Response - Sirona
Urgent Urology Pathway
Acute Prostatitis
Urology A&G Service
Bladder & Bowel Self Care App
Bladder & Bowel Services
Chronic Prostatitis
Circumcision in adults
Erectile Dysfunction
Female Urinary Incontinence
Haematospermia
Haematuria
Hydrocele
LUTS in men
Mesh complications
Overactive Bladder
Penile Disorders
Prostate - including PSA
Renal Calculi
Scrotal Swellings & Testicular Lumps & Pain
Sterile Pyuria
Trial Without Catheter (TWOC)
Urgent Care and Admissions (Urology) - under review
Urinary Tract Infections
Urodynamics
UTIs in Care Homes
Varicocele
Vasectomy
Vascular A&G Service
Aortic Dissection
Arterial Leg Ulcers
Carotid Artery Stenosis
NHS Health Check
Varicose Veins and Venous Leg Ulcers
Vascular Nurse Specialist Clinic
Peripheral Arterial Disease
Vascular Hot Clinic
Abdominal Aortic Aneurysm
Digital Weight Management
Low Calorie Diet Pilot
Non-diabetic Hyperglycaemia and the National Diabetes Prevention Program (NDPP)
Post Bariatric Surgery Monitoring
Weight Management - Tirzepatide (Mounjaro)
Introduction & Tier 1 Weight Management Services
Tier 2 Weight Management Services - BNSSG
Tier 3 & 4 Weight Management Service - BNSSG
Advice & Guidance - Dermatology
Benign skin lesions in children
Community Dermatology Services
Dermoid Cysts
Eczema
IgA Vasculitis (Previously Henoch-Schonlein Purpura)
Pilomatricoma
Nappy Rash
Developmental impairment
Dyspraxia / DCD in children
Faltering Growth
Motor Disorders
Neonatal milk & vitamin guideline
Sleep Disorders
Speech and Language Therapy
Paediatric Nutrition and Dietetic Service
PICA (eating non-edible items)
Avoidant and Restrictive Food Intake Disorder (ARFID)
Audiology
Bell's Palsy
Cleft lip and / or palate
Ear wax in children
ENT HOT Clinic (paediatric)
Epistaxis
Middle ear problems
Motion sickness
Moulded Ear Plugs
Nasal problems
Sleep Apnoea in Children
Sore throat
Speech & Language
Tongue Tie
Tonsils and Adenoids
Chronic Abdominal Pain and IBD
Coeliac disease (children)
Constipation
Diarrhoea and vomiting
Faltering Growth
Milk Related Problems
Neonatal milk & vitamin guideline
Reflux Disease
Helicobacter Pylori (H-Pylori)
Chicken Pox - parents guide
Feverish illness
Lymphadenopathy (Benign) in Children
Respiratory tract infections
Scarlet Fever/ Group A Strep
Asylum & Refugee Clinic (ARC)
Mental Health Resources for Children and Young People
CAMHS mental health 24/7 emergency line
CAMHS Referral information
HappyMaps
Self-harm in Children and Young People
Hep B vaccine for at risk infants
Jaundice
Neonatal milk & vitamin requirements
Sacral dimples and pits
Umbilical Granuloma
Bell's Palsy
Febrile Convulsions
Fits, Faints and Funny Turns
Headache
Head injury
Neuromuscular
Neurosurgery
Tics and Tourette's in children
Back pain
Hip Dysplasia
Limping - acute limp in children
Lower Limb
Scoliosis
Urgent & Non-urgent Referrals
Accurx templates for CYP
Bronchiolitis - parents guide
Chicken Pox - parents guide
Common Childhood Illness - HandiApp
Constipation - A guide for parents
Cough - parent information
Croup - parents guide
Diarrhoea and vomitting - parents guide
Febrile Convulsions - parents guide
Feverish Illness - parents guide
Gastro-oesophageal Reflux - parents guide
Head Injury - parents guide
Healthier Together - Parent Advice
Increasing Iron Intake
Sore Throat - parents guide
Swallowing Pills Advice
Umbilical Granuloma - parents guide
Vulvovaginitis
Weaning to a Cows milk free diet
Wheezy action plan
Advice & Guidance - Respiratory
Asthma in Children- acute (including wheeze)
Asthma in Children - Chronic
Bronchiolitis
Community Acquired Pneumonia
Cough (including PBB)
Croup
Sleep Apnoea in Children
Tuberculosis (children)
BNSSG Safeguarding Team & Training
Referrals & Procedures
Be Safe
Support for children
Children in Care and Care Leavers (also known as Looked After Children)
ADHD Care Pathway for school age children
Auditory Processing Disorder (APD)
Autism spectrum disorder (ASD)
Dyslexia
Early Years Support Practitioner (SEND) Service (BRISTOL)
SEND
Sleep in children and young people
Stop over medication (STAMP)
Breast Symptoms in Children
Burns (children)
Chest Wall Deformity
Hernias in Children
Paediatric Surgery Inc. Urology
Umbilical Granuloma
Assessment of acutely unwell children
Common Urgent Care Conditions
Rapid Access Clinic
Septicaemia (children)
Urgent Care Referrals
Urgent Orthopaedic Referrals
Circumcision in children
Continence
Hydrocele (paediatric)
Penis abnormalities in children
Surgery & Urology
Urinary Tract Infections
Varicocele
Abscesses, Boils and Carbuncles (DRAFT)
Advice & Guidance Services (DRAFT)
Domestic Violence and Abuse (DRAFT)
Support for children (DRAFT)
Anaemia in Pregnancy _ Draft
Avascular Necrosis of Femoral Head - Draft
Back pain/ Spinal pathway - Draft
Catheter Maintenance - Draft
Cauda Equina Syndrome - DRAFT
Cervical Conditions (DRAFT)
Community Urology Service - GP Care (DRAFT)
Consumer Genetic Testing - DRAFT
Family History of Breast and Ovarian Cancer (DRAFT)
Fibroids (DRAFT)
Hyperemesis Gravidarum DRAFT
Menstrual Disorders - (DRAFT)
Muscle Cramps - Draft
Needlestick injury - DRAFT
Neurosurgery - DRAFT
Obsolete pathways
Ovarian Conditions - (DRAFT)
Paediatric Rheumatology - Draft
Papilloedema - Draft
PCOS (DRAFT)
Phlebotomy (DRAFT)
Pyogenic Granuloma - Draft
Raised inflammatory Markers - Draft
Sexually Transmitted Infections - guide to swabs - DRAFT
Shared Decision Making DRAFT
Surgery A&G Services - DRAFT
TEST
Vaccinations (DRAFT)
Vascular Hot Clinic - DRAFT
Vitamin B12 - interim guidelines DRAFT
Reconstructive Prosthetics - DRAFT
Advice & Guidance Services (DRAFT) (v.2)
PREVENT (DRAFT)
Adult Safeguarding (DRAFT)
Ketamine Bladder - Draft
Asthma in Children - Chronic (DRAFT)
Referrals & Procedures (DRAFT)
Be Safe and Youth Inclusion Support Project (DRAFT)
Female Urinary Incontinence (DRAFT)
BNSSG Safeguarding Team & Training (DRAFT)
BNSSG Safeguarding Team & Training (DRAFT) (V2)
Hyperbilirubinaemia - DRAFT
Dyspepsia in children - DRAFT
Vaginal Discharge - Draft
Halitosis - Draft
Infectious Vaginitis (DRAFT)
Formulary Process
Joint Formulary Paperwork
Purpose and Format of the Joint Formulary
The Traffic Light System and Classification of Medicines
Non-formulary and Unlicensed Medicines
Biosimilars
Shared Care
Meeting dates
APMOC Paperwork
1. Gastro-Intestinal System
2. Cardiovascular System
3. Respiratory System
4. Central Nervous System
5. Infections
6. Endocrine System
7. Obstetrics, Gynaecology and Urinary-tract Disorders
8. Malignant Disease and Immunosuppression
9. Nutrition and Blood
10. Musculoskeletal and Joint Diseases
11. Eye
12. Ear, Nose and Oropharynx
13. Skin
14. Immunological Products and Vaccines
15. Anaesthesia
16. Palliative Care
17. Miscellaneous Preparations
1. Gastro–intestinal System Guidelines
2. Cardiovascular System Guidelines
3. Respiratory System Guidelines
4. Central Nervous System Guidelines
5. Infections Guidelines
6. Endocrine System Guidelines
7. Obstetrics, Gynaecology and Urinary-tract Disorders Guidelines
8. Malignant Disease and Immunosuppression Guidelines
9. Nutrition and Blood Guidelines
10. Musculoskeletal and Joint Diseases Guidelines
11. Eye Guidelines
12. Ear, Nose and Oropharynx Guidelines
13. Skin Guidelines
14. Immunological Products and Vaccines Guidelines
16. Palliative Care Guidelines
17. Polypharmacy
18. Care Homes
19. Other
20. Appliances and Part IX
Botulinum Toxin A Pathways
Community Pharmacy Minor Ailment PGDs
Healthcare professionals working in primary care PGDs
NHSE PGDs
BNSSG-wide PGD Policy and Process
BNSSG PGD templates
Medicines Quality and Safety
Adding a Drug to EMIS Web as a 'Hospital Issue'
World Patient Safety Day
Formulary Process
Joint Formulary Paperwork
Purpose and Format of the Joint Formulary
The Traffic Light System and Classification of Medicines
Non-formulary and Unlicensed Medicines
Shared Care
APMOC Paperwork
1. Gastro-intestinal System
2. Cardiovascular system
3. Respiratory System
4. Nervous system
5. Infections
6. Endocrine system
7. Obstetrics, gynaecology, and urinary-tract disorders
8. Malignant Disease and Immunosuppression
9. Nutrition and Blood
10. Musculoskeletal and joint diseases
11. Eye
12. Ear, Nose and Oropharynx
13. Skin
14. Immunological products and vaccines
15. Anaesthesia
16. Palliative Care
17. Miscellaneous Preparations
1. Gastro–intestinal system Guidelines
3. Respiratory System Guidelines
4. Nervous System Guidelines
5. Infections Guidelines
6. Endocrine system Guidelines
9. Blood and nutrition Guidelines
13. Skin Guidelines
20. Appliances and Part IX
Specialist Falls Service
South Glos - Memory Service & Dementia Support
Assistive Technology Service
Pain clinic - NBT
Back Pack - NBT
NBT - Cognitive Disorders Clinic
Endocrinology NBT
Arts on Referral for Chronic Pain - NBT
Falls Service : NBT
Neuropsychiatry Sleep Disorders clinic - NBT
Arts on Referral for Neuromuscular Condition - NBT
Bristol - Psychosis Early Intervention
South Glos - Psychosis Early Intervention
North Somerset - Psychosis Early Intervention
Primary Care Liaison Service
Alkaline Phosphatase
Clinical Biochemistry in Primary Care
Creatinine Kinase
Hyperkalaemia
Hyperlipidaemia
Hypomagnesaemia
Lipid A&G Service
Breast A&G Service
Axillary masses
Breast Implants (non-cancer)
Breast Pain
Breast Surgery
Breastfeeding
Family History of Breast Cancer
Male Breast Symptoms
Mastitis and Breast Abscess
Nipple conditions
Bowel Cancer Screening
Breast Cancer Screening
Cervical Cancer Screening
Pancreatic Cancer Surveillance Programme
Lung Cancer Screening (LCS)
Cancer Support A&G Service
Cancer and Severe Mental Illness (SMI)
LD & Cancer
Living with and beyond cancer (LWBC)
Nutrition in cancer
Physio for NBT Cancer patients
Post cancer - Digital Remote Monitoring and Personalised Stratified Follow Up
Exercise programmes for people affected by cancer
Toxicity Risk Assessment Tool
Cardiology A&G Services
Angina
Arrhythmia
Atrial Fibrillation and Flutter
Cardiac Rehabilitation
Cardiac Rhythm Analysis
Coronary Artery Calcification
ECG - Open Access
ECHO - requesting
Heart Failure
Hypertension
Infective Endocarditis
Inherited Cardiac Conditions
NT Pro BNP Testing
Pacemakers
Postural Orthostatic Tachycardia Syndrome (PoTS)
Pulmonary Hypertension
Rapid Access Chest Pain Clinics
Syncope and TLOC (non-traumatic)
Thoracic Aorta Disease
Care of the Elderly A&G Service
Assistive Technology Service
Falls & Balance
Fracture Liaison Service
Frailty
Hearing Services
Live Longer Better
Movement Disorders
NHS@home - Frailty pathway
Rapid Assessment Clinic For Older People
Referral pathways for older people
Acute Assessment
COVID Medicine Delivery Unit (CMDU)
COVID Oximetry @ Home Virtual Ward
COVID Testing
Long COVID
TeamNet and Latest updates
Dementia - Assessment & referral
Dementia Prescribing
Mental Capacity & Best Interest Decisions
Mild Cognitive Impairment (MCI)
Acne vulgaris
Actinic Keratoses
Dermatology A&G Services
Alopecia
Basal Cell Carcinoma
Benign Skin Lesions
Bowen's Disease
Community Dermatology Service
Cosmetic skin treatments
Eczema
Hidradenitis Suppurativa
Hyperhidrosis
Leg Ulcer
Mole Mapping/Surveillance
Pityriasis Rosea
Pityriasis Versicolor
Polymorphic Light Eruption
Pruritis
Psoriasis
Rosacea
Scabies
Seborrhoeic Dermatitis
Skin Camouflage
Tinea
Tissue Viability/Wound Care Service
Appearance-Related Concerns
Urticaria
Vulval Skin Care
Warts and Verrucas
Community Diabetes Specialist Service
Diabetes & Nutrition
Diabetes A&G Services
Diabetes Foot Care
Diabetes Mellitus - Guidelines
Diabetes self-management
Diabetes Structured Education
Diabetic Eye Screening
Monogenic Diabetes
Neuropathic Pain (Diabetic)
Non-diabetic Hyperglycaemia and the National Diabetes Prevention Program
Pregnancy and diabetes
Rapid Access Diabetes Clinic
Type 2 diabetes management
Type 2 Path to Remission Programme
Dietetics & Nutrition A&G Service
Local Services
Malnutrition & Oral Nutritional Supplements
Vitamin D Deficiency
Weight management
Alcohol Misuse
Opiate Dependence
Non-opiate drug dependence
North Somerset Drug & Alcohol Service
South Gloucestershire Drug & Alcohol Service
Bristol Drug and Alcohol Service
Bristol Primary Care Liaison (formerly Shared Care)
Bereavement support
Death Certification and Medical Examiner
End of Life Care
End of life care - community support
ReSPECT Plus
SR1 Form (formerly DS1500)
St Peters Hospice
Weston Hospice
Adrenal incidentaloma
Adrenal insufficiency
Endocrinology A&G Service
Endocrinology Services - UHBW and NBT
Gynaecomastia
Hirsutism
Hyperprolactinaemia
Hyperthyroidism
Hyponatraemia
Hypothyroidism
Male hypogonadism
Managing glucocorticoid withdrawal
Polyuria
Primary hyperparathyroidism (PHPTH)
Secondary hypertension
Sub Clinical hyperthyroidism
Sub Clinical hypothyroidism
Thyroid Disease and pregnancy
Thyroid eye disease
ENT A&G Service
Anosmia
Audiology (adult)
Dizziness and Vertigo
Ear wax and microsuction
ENT HOT Clinic
Epistaxis
Hearing Problems
Middle ear problems
Moulded Ear Plugs
Nasal Treatment
Neck Lumps (including Goitre)
Otitis Externa
Rhinosinusitis & Nasal Polyps
Snoring
Speech & Language
Tinnitus
Tonsils
Uvula
Advice and Guidance - Gastroenterology and Colorectal Surgery
Anaemia (Iron Deficiency)
Anal FIssure
Barrett's oesophagus
Coeliac Disease
Colon Polyps
Community Gastroenterology Clinic - InHealth
Constipation in Adults
Diverticular Disease
Dyspepsia and Reflux
Endoscopy
Eosinophilic Oesophagitis
Faecal Calprotectin
FIT (Faecal Immunochemical Test)
Gallstones (and polyps)
Haemorrhoids and anal lesions
Hiccups
Inflammatory Bowel Disease (Confirmed)
Inflammatory Bowel Disease (suspected)
Irritable Bowel Syndrome
Microscopic Colitis
Pancreatitis (Acute)
Pancreatitis (Chronic) and PEI
Rectal Bleeding
Stoma care
Upper GI Bleed
Urgent Gastroenterology Services
Alpha 1 Antitrypsin Deficiency (AATD)
Family History of Colorectal Cancer
Genetic Haemochromatosis
Genetics - general
Lynch Syndrome
Monogenic Diabetes
Family History of Breast/Ovarian Cancer
Abnormal Vaginal Bleeding
Gynaecology A&G Service
Cervical Conditions
Dyspareunia
Early Pregnancy Assessment Clinic
Emergency Gynaecology
Endometriosis
Female Cosmetic Surgery
Female Genital Mutilation
Female Genitalia Surgery
Female Urinary Incontinence
Fibroids
Hyperemesis Gravidarum
Menopause
Menstrual Disorders
Mesh Complications
Open Access Gynae Imaging
Ovarian Conditions
PCOS
Pelvic Inflammatory Disease
Pelvic Organ Prolapse
Persistent Pelvic Pain (women)
Premature Ovarian Insufficiency
Recurrent Miscarriage
Termination of Pregnancy
Vulval Skin Conditions
Haematology A&G Service
Anaemia
Blood Transfusions & Iron infusions
Genetic Haemochromatosis
Guidelines for Primary Care
Leucocytosis (including neutrophilia and lymphocytosis)
Lymphadenopathy (adults)
Macrocytosis
Polycythaemia
Sickle Cell & Thalassaemia
Vitamin B12
Warfarin monitoring
Hepatology A&G Service
Genetic Haemochromatosis
Liver disease
Urgent Hepatology Service
Viral Hepatitis
Advice & Referrals - Infectious Diseases and Microbiology
Antimicrobial Guidelines (Primary Care)
Clostridioides difficile in the community
COVID -19 (Coronavirus)
Group A Strep
Helicobactor Pylori
Immunisation Schedules
Infection Sciences Test Sample Quick Guide
Influenza
Lyme Disease
Malaria
Measles
Mpox
Mumps
Public Health and Notifiable Diseases
Syphilis
Tuberculosis
Varicella
Vector Borne Diseases
Viral Haemorrhagic Fever (incl Ebola)
Whooping Cough
Middle Eastern Respiratory Virus - MERS-CoV
Biochemistry Advice
Chronic Disease Monitoring
Community Diagnostic Centres
Community phlebotomy
Inflammatory Marker Testing
Medical Calculators
Transport and storage of samples
Pathology Services
Adult Learning Disability Health Service
Constipation and Learning Disability
Dyslexia
Dyspraxia / DCD in adults
LD & Autism Hospital Liaison
LD & Cancer Screening
LeDeR - learning disability mortality reviews
Mental Capacity & Best Interest Decisions
Resources for Learning Disability Annual Health Checks and Health Action Plans
Stop over medication (STOMP)
Max Fax and Dental A&G Service
Cleft Lip and/or Palate (adult)
Dental Care
Reconstructive Prosthetics Services
Salivary Gland Problems
Temporomandibular Joint Disorders
Trigeminal Neuralgia
Alternatives and Adjuncts to HRT
Cardiovascular conditions and HRT
Contraception and Menopause
Diagnosing menopause
Early menopause - under 45
Genitourinary symptoms
Gynaecology conditions and HRT
Hormone Replacement Therapy (HRT)
HRT and breast conditions
HRT and Migraines
HRT in over 60s
Hormone sensitive cancers
Post-menopausal bleeding - not on HRT
Premature Ovarian Insufficiency (Menopause <40y)
Referral - Menopause
Side effects and risks of HRT
Testosterone for low libido
Unscheduled bleeding on HRT
VTE and HRT
Resources for patients
24/7 Mental Health Support
ADHD (adult)
Autism-Spectrum
Depression (adults)
Eating Disorders
Gambling Addiction
HOPE programme
ICU Follow-up NBT
Insomnia
MINT (Mental health and wellbeing Integrated Network Team)
Mental Health - Social Prescribing
Mental Health Support - Which Service
Neuropsychiatry
Perinatal Mental Health
Primary Care Liaison Service - AWP
Psychosis: Schizophrenia
Safe Haven Mental Health Support
Sanctuary (Bristol) Mental Health Support
Second Step Wellbeing Services
Self Harm
Self-help Leaflets for Mental Health
Sexual Assault / Abuse Support
SMI (Severe Mental Illness) Physical Health Improvement
Suicidal Thoughts
Talking Therapies (IAPT)
Coping With Appearance Concerns
Veterans Mental Health
Right to Choose (ADHD/ASD Patient Choice)
Nephrology A&G Service
Acute Kidney Injury
Chronic Kidney Disease
Renal referrals (including urgent referrals)
Neurology/HOT Clinic A&G Service
Neurovascular/Stroke A&G Service
Bell's Palsy
Cognitive Disorders
Concussion / mild traumatic brain injury
First Seizure Clinic
Head Injury Therapy Unit
Headache (adults)
Huntington's Disease
Multiple Sclerosis
Neuromuscular
Neurophysiology
Neuropsychiatry
Parkinson's Disease
Peripheral Neuropathy- Under Review
Restless Leg Syndrome
Spasticity service
Specialist Community Neurology
Stroke
Transient Ischaemic Attack
Tremor
Trigeminal Neuralgia
Neurosurgical Referrals - General
Arachnoid cysts
Brain Conditions
Cauda Equina Syndrome
Epilepsy surgery and DBS
Normal Pressure Hydrocephalus
Peripheral Nerve Conditions
Spinal Conditions
Subdural Haematoma
Trigeminal Neuralgia
Obstetrics A&G Service
Cholestasis of Pregnancy
Diabetes in Pregnancy
Early Pregnancy Assessment Clinic
Family Nurse Partnership
Folic acid and Vitamin B12 in pregnancy
Group B Strep in Pregnancy
Hyperemesis Gravidarum
Hypertension in pregnancy
Maternity Services
Perinatal Mental Health
Post Natal Care
Termination of pregnancy
Thyroid Disease and Pregnancy
Vaccination in Pregnancy
Acute Angle Closure Glaucoma
Ophthalmology A&G Service
Allergic Eye Disease
Anterior Uveitis / Iritis
Blepharitis
Cataract
Chalazion & Styes
Chemical injury
Conjunctivitis
Contact Lens Related Keratitis (Corneal Ulcer)
Corneal Abrasion
Corneal Foreign Body
Dry Eye
Endophthalmitis
Episcleritis
Eyelid conditions
Floaters & Flashes
Giant Cell Arteritis
Glaucoma
Hyphaema
Low Vision
Neuro-ophthalmology
Open Eye Injury
Ophthalmic Shingles
Orbital Trauma / Suspected Orbital Fracture
Pingueculum & Pterygium
Pre-septal and Post-septal Cellulitis
Referral Guidance & Tips
Subconjunctival Haemorrhage
Urgent Ophthalmology Referrals
Acute knee & shoulder clinics
Orthopaedics A&G Service
Back pain/ Spinal pathway
Carpal Tunnel Syndrome
Dupuytren's Contracture
Foot and Ankle Problems
Fracture Clinics
Funding Policies for Orthopaedics
Ganglion
getUBetter app
Hand problems
Hip Pain
Knee Pain
Meralgia Paraesthetica
MSK Foot & Ankle service
Musculoskeletal (MSK) self-help
Musculoskeletal Interface (MSKI) Service
Periprosthetic hip infection
Shoulder Problems
Sports Injuries
Steroid injections
Trigger Finger
Acupuncture
Pain Management A&G Service
Back Pack
Fibromyalgia
ME/Chronic Fatigue Syndrome
Persistent (Chronic) pain
Spinal Cord Stimulation Service
Physiotherapy A&G Service
Divarication of Recti
MSK Physio services
Neurophysiotherapy
Pelvic Health Physio
Respiratory Physio
Self-management Hip & Knee pain
Alternative Medicine
Antibiotics
Cannabis prescribing
Community Pharmacy
Hosiery
Medication to avoid in dementia patients
Medicines for Self Care
Medicines Quality and Safety
NHS@Home - IV antimicrobials (OPAT)
Opioid Conversion
Prescribing in pregnancy and breastfeeding
Psychotropic Medication Monitoring
Toxbase
Vitamin D
Advice & Queries
Direct Access Radiology (adults)
ICE System for Radiology (& Pathology) Referrers
Image Guided Steroid Injections
MRI considerations
Radiology Guidelines for Primary Care
Spinal Imaging in Primary Care
Ultrasound guidance
Respiratory A&G Service
Air pollution and health
Asthma (adults)
Breathing Pattern Disorders
Bronchiectasis
Chronic Breathlessness Support
Chronic cough
Chronic Obstructive Pulmonary Disease
Community Respiratory Service
Fit to Fly Assessments
Home oxygen ordering
HOT Clinics (Respiratory)
Interstitial Lung Disease
Long-term Ventilation (LTV) Service
myCOPD App
NHS@home - Respiratory pathway
Obstructive Sleep Apnoea
Pleural Services
Pulmonary Rehabilitation
Respiratory Triage Services (RAS)
Smoking Cessation
Spirometry and Lung Function Tests
Tuberculosis
Lung Cancer Screening (LCS)
Rheumatology A&G Service
Axial Spondyloarthritis (including ank spond)
Early Inflammatory Arthritis
Fibromyalgia
Giant Cell Arteritis
Gout (Crystal Arthropathy)
Hypermobility and EDS
Osteoporosis
Osteoporotic Vertebral Fracture
Polymyalgia Rheumatica (PMR)
Psoriatic Arthritis (PsA)
Raynaud's Phenomenon
Sjorgren's Sydrome
Systemic Lupus Erythematous
Young Adult Rheumatology Service
Adult Safeguarding
BNSSG Safeguarding Team & Training
Domestic Violence and Abuse
Sexual assault/ abuse support
PREVENT
Better Health North Somerset
Exercise on referral
HOPE programme
Live Longer Better
Musculoskeletal (MSK) self-help
South Gloucestershire
Self Care
Smoking Cessation
Sexual Health A&G Service
Chronic Pelvic Pain Syndrome (men)
Contraception
Emergency Contraception
Gonorrhoea
HIV
LARC
LARC Complex referrals
Loss of Libido
Mpox
Pelvic Inflammatory Disease
Post Birth Contraception
Psychosexual Service
Sexual assault/ abuse support
Sexual Health Guidelines and Referral
Syphilis
Circadian Rhythm Disorder
Insomnia
Obstructive Sleep Apnoea (OSA)
Parasomnias
Primary Hypersomnias
Restless Leg Syndrome
Advice & Guidance Service
Cosmetic Treatment (including scar revision)
Foreign Body Removal (soft tissue)
Hernias (adults)
Burns (adult)
Pre-operative assessment
Reconstructive Prosthetics Services
Surgical Emergency Care
Admission protocols
Dementia Wrap Around Care - North Somerset
Frailty - ACE
Frailty - Urgent Care
HOT Clinics & Rapid Access
Live UEC Dashboard
Medical Assessment/Admission and Weekday IUC Professional Line
NHS@home
Septicaemia (adults)
Sirona Professional Lines
Surgical Emergency Care
Transport to Hospital
Urgent Care, MIU & WIC
Urgent Community Response - Sirona
Urgent Urology Pathway
Acute Prostatitis
Urology A&G Service
Bladder & Bowel Self Care App
Bladder & Bowel Services
Chronic Prostatitis
Circumcision in adults
Erectile Dysfunction
Female Urinary Incontinence
Haematospermia
Haematuria
Hydrocele
LUTS in men
Mesh complications
Overactive Bladder
Penile Disorders
Prostate - including PSA
Renal Calculi
Scrotal Swellings & Testicular Lumps & Pain
Sterile Pyuria
Trial Without Catheter (TWOC)
Urgent Care and Admissions (Urology) - under review
Urinary Tract Infections
Urodynamics
UTIs in Care Homes
Varicocele
Vasectomy
Vascular A&G Service
Aortic Dissection
Arterial Leg Ulcers
Carotid Artery Stenosis
NHS Health Check
Varicose Veins and Venous Leg Ulcers
Vascular Nurse Specialist Clinic
Peripheral Arterial Disease
Vascular Hot Clinic
Abdominal Aortic Aneurysm
Digital Weight Management
Low Calorie Diet Pilot
Non-diabetic Hyperglycaemia and the National Diabetes Prevention Program (NDPP)
Post Bariatric Surgery Monitoring
Weight Management - Tirzepatide (Mounjaro)
Introduction & Tier 1 Weight Management Services
Tier 2 Weight Management Services - BNSSG
Tier 3 & 4 Weight Management Service - BNSSG
Advice & Guidance - Dermatology
Benign skin lesions in children
Community Dermatology Services
Dermoid Cysts
Eczema
IgA Vasculitis (Previously Henoch-Schonlein Purpura)
Pilomatricoma
Nappy Rash
Developmental impairment
Dyspraxia / DCD in children
Faltering Growth
Motor Disorders
Neonatal milk & vitamin guideline
Sleep Disorders
Speech and Language Therapy
Paediatric Nutrition and Dietetic Service
PICA (eating non-edible items)
Avoidant and Restrictive Food Intake Disorder (ARFID)
Audiology
Bell's Palsy
Cleft lip and / or palate
Ear wax in children
ENT HOT Clinic (paediatric)
Epistaxis
Middle ear problems
Motion sickness
Moulded Ear Plugs
Nasal problems
Sleep Apnoea in Children
Sore throat
Speech & Language
Tongue Tie
Tonsils and Adenoids
Chronic Abdominal Pain and IBD
Coeliac disease (children)
Constipation
Diarrhoea and vomiting
Faltering Growth
Milk Related Problems
Neonatal milk & vitamin guideline
Reflux Disease
Helicobacter Pylori (H-Pylori)
Chicken Pox - parents guide
Feverish illness
Lymphadenopathy (Benign) in Children
Respiratory tract infections
Scarlet Fever/ Group A Strep
Asylum & Refugee Clinic (ARC)
Mental Health Resources for Children and Young People
CAMHS mental health 24/7 emergency line
CAMHS Referral information
HappyMaps
Self-harm in Children and Young People
Hep B vaccine for at risk infants
Jaundice
Neonatal milk & vitamin requirements
Sacral dimples and pits
Umbilical Granuloma
Bell's Palsy
Febrile Convulsions
Fits, Faints and Funny Turns
Headache
Head injury
Neuromuscular
Neurosurgery
Tics and Tourette's in children
Back pain
Hip Dysplasia
Limping - acute limp in children
Lower Limb
Scoliosis
Urgent & Non-urgent Referrals
Accurx templates for CYP
Bronchiolitis - parents guide
Chicken Pox - parents guide
Common Childhood Illness - HandiApp
Constipation - A guide for parents
Cough - parent information
Croup - parents guide
Diarrhoea and vomitting - parents guide
Febrile Convulsions - parents guide
Feverish Illness - parents guide
Gastro-oesophageal Reflux - parents guide
Head Injury - parents guide
Healthier Together - Parent Advice
Increasing Iron Intake
Sore Throat - parents guide
Swallowing Pills Advice
Umbilical Granuloma - parents guide
Vulvovaginitis
Weaning to a Cows milk free diet
Wheezy action plan
Advice & Guidance - Respiratory
Asthma in Children- acute (including wheeze)
Asthma in Children - Chronic
Bronchiolitis
Community Acquired Pneumonia
Cough (including PBB)
Croup
Sleep Apnoea in Children
Tuberculosis (children)
BNSSG Safeguarding Team & Training
Referrals & Procedures
Be Safe
Support for children
Children in Care and Care Leavers (also known as Looked After Children)
ADHD Care Pathway for school age children
Auditory Processing Disorder (APD)
Autism spectrum disorder (ASD)
Dyslexia
Early Years Support Practitioner (SEND) Service (BRISTOL)
SEND
Sleep in children and young people
Stop over medication (STAMP)
Breast Symptoms in Children
Burns (children)
Chest Wall Deformity
Hernias in Children
Paediatric Surgery Inc. Urology
Umbilical Granuloma
Assessment of acutely unwell children
Common Urgent Care Conditions
Rapid Access Clinic
Septicaemia (children)
Urgent Care Referrals
Urgent Orthopaedic Referrals
Circumcision in children
Continence
Hydrocele (paediatric)
Penis abnormalities in children
Surgery & Urology
Urinary Tract Infections
Varicocele
Abscesses, Boils and Carbuncles (DRAFT)
Advice & Guidance Services (DRAFT)
Domestic Violence and Abuse (DRAFT)
Support for children (DRAFT)
Anaemia in Pregnancy _ Draft
Avascular Necrosis of Femoral Head - Draft
Back pain/ Spinal pathway - Draft
Catheter Maintenance - Draft
Cauda Equina Syndrome - DRAFT
Cervical Conditions (DRAFT)
Community Urology Service - GP Care (DRAFT)
Consumer Genetic Testing - DRAFT
Family History of Breast and Ovarian Cancer (DRAFT)
Fibroids (DRAFT)
Hyperemesis Gravidarum DRAFT
Menstrual Disorders - (DRAFT)
Muscle Cramps - Draft
Needlestick injury - DRAFT
Neurosurgery - DRAFT
Obsolete pathways
Ovarian Conditions - (DRAFT)
Paediatric Rheumatology - Draft
Papilloedema - Draft
PCOS (DRAFT)
Phlebotomy (DRAFT)
Pyogenic Granuloma - Draft
Raised inflammatory Markers - Draft
Sexually Transmitted Infections - guide to swabs - DRAFT
Shared Decision Making DRAFT
Surgery A&G Services - DRAFT
TEST
Vaccinations (DRAFT)
Vascular Hot Clinic - DRAFT
Vitamin B12 - interim guidelines DRAFT
Reconstructive Prosthetics - DRAFT
Advice & Guidance Services (DRAFT) (v.2)
PREVENT (DRAFT)
Adult Safeguarding (DRAFT)
Ketamine Bladder - Draft
Asthma in Children - Chronic (DRAFT)
Referrals & Procedures (DRAFT)
Be Safe and Youth Inclusion Support Project (DRAFT)
Female Urinary Incontinence (DRAFT)
BNSSG Safeguarding Team & Training (DRAFT)
BNSSG Safeguarding Team & Training (DRAFT) (V2)
Hyperbilirubinaemia - DRAFT
Dyspepsia in children - DRAFT
Vaginal Discharge - Draft
Halitosis - Draft
Infectious Vaginitis (DRAFT)
Formulary Process
Joint Formulary Paperwork
Purpose and Format of the Joint Formulary
The Traffic Light System and Classification of Medicines
Non-formulary and Unlicensed Medicines
Biosimilars
Shared Care
Meeting dates
APMOC Paperwork
1. Gastro-Intestinal System
2. Cardiovascular System
3. Respiratory System
4. Central Nervous System
5. Infections
6. Endocrine System
7. Obstetrics, Gynaecology and Urinary-tract Disorders
8. Malignant Disease and Immunosuppression
9. Nutrition and Blood
10. Musculoskeletal and Joint Diseases
11. Eye
12. Ear, Nose and Oropharynx
13. Skin
14. Immunological Products and Vaccines
15. Anaesthesia
16. Palliative Care
17. Miscellaneous Preparations
1. Gastro–intestinal System Guidelines
2. Cardiovascular System Guidelines
3. Respiratory System Guidelines
4. Central Nervous System Guidelines
5. Infections Guidelines
6. Endocrine System Guidelines
7. Obstetrics, Gynaecology and Urinary-tract Disorders Guidelines
8. Malignant Disease and Immunosuppression Guidelines
9. Nutrition and Blood Guidelines
10. Musculoskeletal and Joint Diseases Guidelines
11. Eye Guidelines
12. Ear, Nose and Oropharynx Guidelines
13. Skin Guidelines
14. Immunological Products and Vaccines Guidelines
16. Palliative Care Guidelines
17. Polypharmacy
18. Care Homes
19. Other
20. Appliances and Part IX
Botulinum Toxin A Pathways
Community Pharmacy Minor Ailment PGDs
Healthcare professionals working in primary care PGDs
NHSE PGDs
BNSSG-wide PGD Policy and Process
BNSSG PGD templates
Medicines Quality and Safety
Adding a Drug to EMIS Web as a 'Hospital Issue'
World Patient Safety Day
Formulary Process
Joint Formulary Paperwork
Purpose and Format of the Joint Formulary
The Traffic Light System and Classification of Medicines
Non-formulary and Unlicensed Medicines
Shared Care
APMOC Paperwork
1. Gastro-intestinal System
2. Cardiovascular system
3. Respiratory System
4. Nervous system
5. Infections
6. Endocrine system
7. Obstetrics, gynaecology, and urinary-tract disorders
8. Malignant Disease and Immunosuppression
9. Nutrition and Blood
10. Musculoskeletal and joint diseases
11. Eye
12. Ear, Nose and Oropharynx
13. Skin
14. Immunological products and vaccines
15. Anaesthesia
16. Palliative Care
17. Miscellaneous Preparations
1. Gastro–intestinal system Guidelines
3. Respiratory System Guidelines
4. Nervous System Guidelines
5. Infections Guidelines
6. Endocrine system Guidelines
9. Blood and nutrition Guidelines
13. Skin Guidelines
20. Appliances and Part IX
Specialist Falls Service
South Glos - Memory Service & Dementia Support
Assistive Technology Service
Pain clinic - NBT
Back Pack - NBT
NBT - Cognitive Disorders Clinic
Endocrinology NBT
Arts on Referral for Chronic Pain - NBT
Falls Service : NBT
Neuropsychiatry Sleep Disorders clinic - NBT
Arts on Referral for Neuromuscular Condition - NBT
Bristol - Psychosis Early Intervention
South Glos - Psychosis Early Intervention
North Somerset - Psychosis Early Intervention
Primary Care Liaison Service
Elevated haemoglobin / haematocrit has a wide differential diagnosis:
The threshold for therapeutic intervention with venesection or cytoreductive therapy in an individual patient depends on the cause, associated symptoms and thrombotic risk factors. For most secondary or relative causes of polycythaemia there is no evidence to support intervention with venesection. Co-existing iron deficiency can sometimes mask the presence of polycythaemia vera.
The JAK2 V617F mutation is detectable in over 95% of patients with PV. Where this mutation is absent, it is a reliable indicator that the patient does not have PV and that secondary causes are implicated.
Indications for testing
*Testing on at least two separate occasions > 3 months apart. Ensure no/minimal tourniquet venostasis for blood samples.
Assessment and Investigations in primary care prior to referral
Assessment:
Investigations in primary care:
Criteria for referral to secondary care:
Management in primary care:
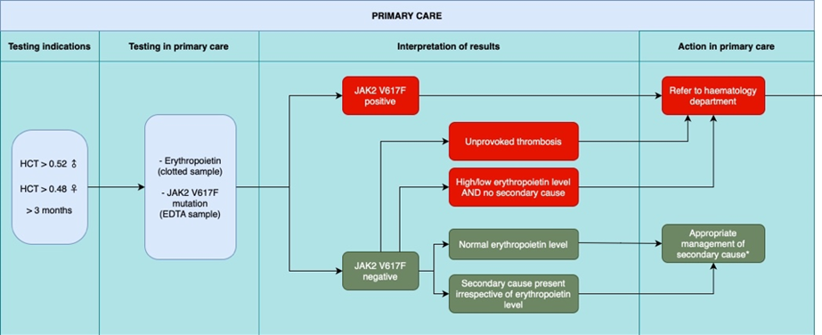
Investigation and management of adult patients presenting with polycythaemia in primary care. From SW MPN Group guideline 2023 Dr Mahdi et al.
Raised haematocrit with:
URGENT ADVICE: 9am to 5pm via hospital switchboard for haematology SpR. ONLY for emergency advice. Out of hours and weekends – emergency advice may be obtained from the on-call haematology clinician via hospital switchboard.
NON-URGENT ADVICE: use Haematology Advice and Guidance service via e-RS. Your query should be responded by a consultant haematologist within 3 working days.
REFERRAL: via e-RS or Haematology - USC (2WW) as indicated.
Minimal information: the referral letter should include abnormal clinical findings (location, size, any associated features) and any abnormal full blood count results or other relevant test results, particularly if these investigations were not done in laboratories of the hospital to which the referral is made.
Other haematology referrals: most new referrals will go to one of the general haematology clinics but may be triaged to a specialist clinic.
BSH guideline - Diagnosis and management of polycythaemia vera 2018: British Journal of Haematology | Wiley Online Library
Efforts are made to ensure the accuracy and agreement of these guidelines, including any content uploaded, referred to or linked to from the system. However, BNSSG ICB cannot guarantee this. This guidance does not override the individual responsibility of healthcare professionals to make decisions appropriate to the circumstances of the individual patient, in consultation with the patient and/or guardian or carer, in accordance with the mental capacity act, and informed by the summary of product characteristics of any drugs they are considering. Practitioners are required to perform their duties in accordance with the law and their regulators and nothing in this guidance should be interpreted in a way that would be inconsistent with compliance with those duties.
Information provided through Remedy is continually updated so please be aware any printed copies may quickly become out of date.